Download Physiology of the Heart Reviewer and more Study notes Human Physiology in PDF only on Docsity!
1
CHAPTER 9: CARDIAC MUSCLE; THE HEART AS A PUMP AND FUNCTION OF THE HEART VALVES
PHYSIOLOGY OF CARDIAC MUSCLE
Three major types of cardiac muscle:
- Atrial muscle
- Ventricular muscle
- Conductive muscle fibers – contract feebly because they contain
a few contractile fibers; exhibit automatic rhythmical electrical
discharge (action potentials)
Syncytium – has syncytial interconnecting nature; beats as one unit
2 Syncytia – separated by AV valves
Atrial – contracts first
Ventricular
AV bundle – conducts action potential
between the two syncytia since AV
valves do not conduct; bundle of
conductive fibers
ACTION POTENTIALS IN CARDIAC MUSCLE
Phase Channel(s) Notes
depolarization
Open Fast Na MP – becomes more positive until +20 mV
Slow open
Slow Ca (T-type)
1 – initial
repolarization
Close Fast Na K
leaves cell thru open K
channels
Open K
Slow open
Slow Ca
2 – plateau Open
L-type Ca/
Ca-Na/Slow Ca
Brief repola occurs
Plateau result as (1) inc Ca
++
permeability;
(2) dec K
permeability
Close K
3 – rapid
repolarization
Open K Inc K
permeability; Dec Ca
++
permeability
Close
Slow Ca
4 – RMP Resting Membrane Potential ave=~-90 mV
Velocity of signal conduction in Cardiac muscle
- Atrial and Ventricular muscle fibers = 0.3 m/s – 0.5 m/s
o
1/250 V large nerve fibers
o
1/50 V skeletal muscle fibers
- Purkinje fibers – specialized conduction system – 4 m/s; allows reasonably rapid
contraction of excitatory signals
Refractory period
- 0.25 to 0.30 sec
- Duration of the prolonged
plateau action potential
refractory period – 0.05 s
during which the muscle is
more difficult to excite
than normal
- Strong excitatory signals
can still excite
2
Calcium ions disperse to the sarcoplasm thru:
- Longitudinal sarcoplasmic reticulum – from thru T-tubule
action potential
- T-tubules at time of action potential – opens Ca
++
gated
channels
a. Ca ions that enter thru T-tubules activates Ca
++
release
channels aka ryanodine receptor channels in sarcoplasmic
reticulum
b. Release of Ca
++
from sarcoplasmic reticulum
o Without Ca
++
from T-tubules, strength of cardiac muscle
is reduced considerably
o Sarcoplasmic reticulum of cardiac muscle is less well
developed; does not store enuf calcium to produce strong
contractions
o T-tubules of cardiac muscle have a diameter 5 times as
great, volume 25 times as great
o Inside the T-tubules – large quantity of
mucopolysaccharides that are electronegatively-charged
and bind abundant stores of calcium ions
The contraction of cardiac muscle depends strongly on the presence and concentration of calcium ions in the ECF
Duration of Contraction
At end of plateau of cardiac action potential, the influx of Ca ions is cut off.
Transport of calcium back to the sarcoplasmic reticulum – achieved using Ca-ATPase pump and Na-Ca exchanger (Na
in cell transported out by
Na-K ATPase pump
Atrial muscle contraction = 0.2 s
Ventricular muscle contraction = 0.3 s
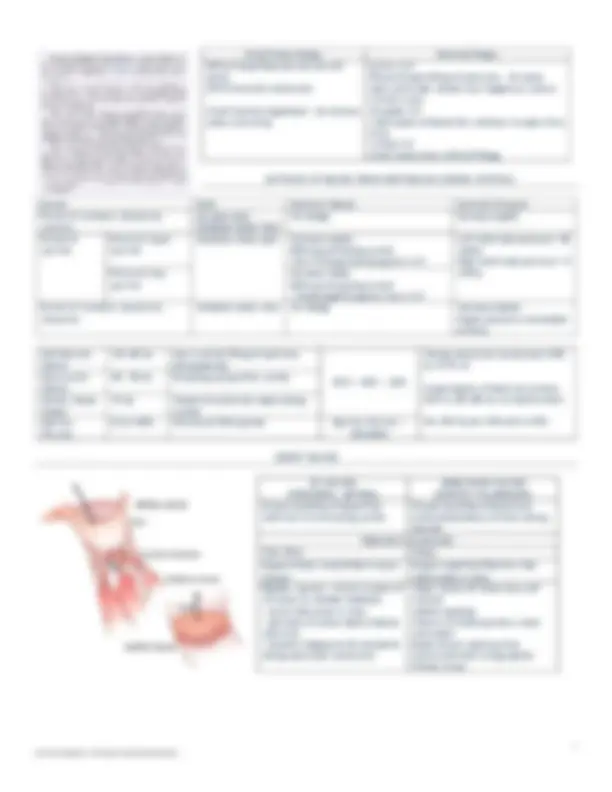
CARDIAC CYCLE
Begins in the sinus node
Atria acts as primer pumps
Ventricles major pumping force
DIASTOLE AND SYSTOLE
Diastole – heart fills with blood
Systole – period of contraction
Duration of 1 cycle =
1
ℎ𝑒𝑎𝑟𝑡 𝑟𝑎𝑡𝑒
Ex. HR = 62 bpm; cycle = 0.0139 mpb
When HR inc, duration dec
Action potential and period of contraction in
systole dec but diastole dec even more
Systole =~ 0.4 of 1 cycle
Diastole = ~0.65 of 1 cycle
This means that the heart beating at a very fast rate
does not remain relaxed long enough to allow complete
filling before contraction starts again
Waves in ECG
Wave Interpretation
P Spread of depolarization thru atria followed by atrial contraction
QRS ~0.16 s after P wave; Electrical depolarization of ventricles; Begins slightly before onset of ventricular systole
T Ventricle repolarization; Occurs slightly before the end of ventricular contraction
U Not always seen; probably represents late repolarization* (not Guyton)
J point – Point immediately after S wave, beginning of ST segment; ST segment – isoelectric area between S and T waves
4
AORTIC PRESSURE CURVES
Entry of blood into the arteries during systole = pressure rises to 120 mmHg
Incisura – occurs in aortic pressure curve when aortic valve closes
- caused by a slight backflow of blood immediately before closure of valve, followed by sudden cessation of backflow
LV, Aorta: 120 mmHg (systolic pressure); 80 mmHg (diastolic pressure)
RV, Pulmonary artery : 20 mmHg (systolic); 14 mmHg (diastolic)
GRAPHICAL ANALYSIS OF VENTRICULAR PUMPING
EW = Net external work output = PxV
Phase Pressure Volume
I: Period of filling 2 - 3 mmHg to 5-7 mmHg 50 mL to 120 mL (EDV)
II: Period of isovolumic contraction 5 - 7 mmHg to 80 mmHg 120 mL
III: Period of ejection 80 mmHg to 120 mmHg to 100 mmHg Decreases to 50 mL
IV: Period of isovolumic relaxation 100 mmHg to 2-3 mmHg 50 mL
Preload – degree of tension on the muscle when it begins to contract; End-diastolic pressure; when ventricle has been filled
Afterload – load against which the muscle exerts its contractile force; pressure in aorta leading from the ventricle
- systolic pressure in phase III
REGULATION OF HEART PUMPING
Rest – 4 to 6 L/min
Strenuous exercise – x4-7 more
VENTRICULAR FUNCTION CURVES
As the atrial pressure for each side of the heart increases, the
stroke work output for that side increases until it reaches the limit
of the ventricle’s pumping ability
Ventricular function curves – another way of expressing the Frank-
Starling mechanism
- Ventricles fill in response to higher atrial pressures
- Each ventricular volume and strength of cardiac muscle contraction
increase, pumping of increased volumes of blood
FRANK-STARLING MECHANISM
Venous return – almost entirely determines amount of blood pumped
each minute
- rate of blood flow from veins to heart
Frank-Starling mechanism – intrinsic ability of the heart to adapt to
increasing volumes of inflowing blood
- the greater the heart is stretched during filling, the greater the
force of contraction, greater amount of blood pumped into aorta
- Within physiological limits, the heart pumps all the blood that
returns to it by way of veins
Stretch of the right atrial wall – increases HR by 10-20%
- helps increase the amount of blood pumped
- smaller contribution than Frank-Starling mechanism
5
Sympathetic nerve inhibition
Decrease cardiac pumping to moderate extent
HR decreased 30% below normal
Strength of ventricular contraction decrease to 30% below normal
Sympathetic stimulation Parasympathetic vagal stimulation
Cardiac output (amount of blood
pumped/min) increased to more than
100% (2-3x in addition to Frank-
Starling mechanism)
Cardiac output decreased to almost 0%
HR increase from 70 bpm to 180- 200
(even 250) bpm
Reduces HR by 20-30%
Increase force of contraction 2x Decreases strength of ventricular
contraction slightly (because vagal
nerves mostly attach to atria)
Increases volume of blood pumped
Increases ejection pressure
Changes in cardiac output are from:
Changes in heart rate
Changes in contractile strength of heart
EFFECT OF POTASSIUM AND CALCIUM IONS
Potassium (X’s)/ Deficiency of Calcium Calcium (X’s)
dilated and flaccid heart, slows HR Causes heart to move towards spastic contraction
Block conduction of cardiac impulse from atria to ventricles via AV
bundle
Initiates contractile process
Elevation of normal values to 8 meq/L – 12 meq/L (2-3x normal value
4 meq/L) can cause severe weakness of the heart, abnormal rhythm,
death
High extracellular [K
] concentration decreases RMP
High extracellular [K
] partially depolarizes cell membrane
EFFECT OF TEMP
High temp inc HR (up to 2x)
Low temp dec HR
Heat inc permeability of the membrane to ions that control the HR
Contractile strength – enhanced temporarily by moderate inc in temp (ie exercise)
INCREASING ARTERIAL PRESSURE LOAD (UP TO A LIMIT) DOES NOT
DECREASE CARDIAC OUTPUT
- No effect until >160 mmHg
- At normal arterial pressures (systolic: 80-140 mmHg), cardiac output is
determined almost entirely by ease of blood flow through body’s tissues (which in
turn controls venous return to heart)
7
INTERNODAL AND INTERATRIAL PATHWAYS CONDUCTION
Velocity of
conduction
Total
delay in
conduction
Notes
Atrial muscle 0.3 m/sec
Small bands of
atrial fibers
1 m/sec 1) connect SA node to AV node:
anterior, posterior, lateral
internodal bands
- connect R atrium to L atrium:
anterior interatrial band
SA node to AV
node
1 m/sec 0.03 s • Slow conduction thru atria due to
diminished number of gap
junctions AV node 1 m/sec 0.09 s
AV node to AV
bundle
(penetrating
portion)
1 m/sec 0.04 s
AV bundle
fibers (distal
portion)
m/sec
- Large muscle fibers
- High level of permeability
between successive gap junctions
at the intercalated discs between
cells
- Few myofibrils – they contract
little or not at all
- Acts as a barrier (one-way
conduction of impulses) – There is
a fibrous barrier
- This prevents re-entry of
impulses back to the atria
AV bundle (5- 15
mm towards
apex) to end of
Purkinje fibers
m/sec
0.03 s
End of Purkinje
fibers to the
rest of
ventricular
muscle
m/sec
0.03 s • Cardiac muscle wraps around the
heart in a double layer, with
fibrous septa between layers
- Cardiac impulse does not travel
directly outwards
- Cardiac impulse travels spirally
towards the direction of how the
muscle wraps around the heart
CONTROL OF EXCITATION AND CONDUCTION
Sinus node – normal pacemaker of the heart (70- 80 x/min)
AV nodal fibers – discharge 40- 60 x/min
Purkinje fibers – discharge 15 – 40 x/min
Why is the SA node the pacemaker?
- It discharges faster than AV and Purkinje
Ectopic pacemakers – abnormal pacemakers
- pacemaker somewhere else in the heart besides the SA node
- causes abnormal contractions
- causes:
may develop faster discharging than SA node
heart blocks/nodal blocks
Stokes-Adams syndrome – delayed pick-up of heartbeat by
Purkinje fibers when there is a nodal block
- delayed pickup caused by desensitization of Purkinje from normal
overdriven SA discharging
- may cause fainting or death
ROLE OF PURKINJE IN SYNCHRONICITY
- causes excitation of ventricular muscles to be in sync (with only
0.03-0.06 s delay)
SYMPA AND PARASYMPA
Parasympathetic Sympathetic
Hormone
released
Acetylcholine Norepinephrine –
stimulates β-I
adrenergic
receptors
Rate of rhythm Decrease Increase
Excitability Decrease at AV junctional
fibers between atrial
musculature and AV node
Increased in all
parts of the heart
Transmission of
cardiac impulse
Decrease Increase
Increased sinus
nodal discharge
Rate of pumping Decreased
Strong – stop; may cause
Purkinje fibers to create
their own rhythm
Increased rate of
conduction
Increased force of
contraction both in
atrium and
ventricles
Permeability to
ions
Increased for potassium
efflux
Increased for
sodium-calcium
permeability
8
CHAPTER 11: NORMAL ELECTROCARDIOGRAM
Electrocardiogram – electric potentials generated by current which are recorded from electrodes on the surface of the body
CHARACTERISTICS:
P wave – electrical potentials generated from atrial depolarization
QRS complex – potentials generated from ventricular depolarization
T wave – potentials generated from ventricular repolarization, occurs 0.25 to
0.35 sec after depolarization
Depolarization waves – normal negative potentials inside the fiber reverses and
becomes positive
Repolarization – positive potentials turn back to become the normal negative resting
potential
Note that only partially depolarized
or partially repolarized muscle fibers
generate current, completely
depolarized or repolarized fibers will
not generate an ECG reading
Current – what flows to the surface
of the body, generated by the
difference in electronegativity in
the fibers
- this is what is picked up by the
electrodes
Interpretation Voltage
10 small lines – 1 mV
Time
1 interval (dark lines) – 0.20 sec
1 interval (thin lines) – 0.04 sec
P wave Beginning of atrial
contraction
0.1 – 0.3 mV PQ/PR interval (0.12-0.2s)*
beginning of QRS complex
QRS complex Beginning of
ventricular contraction
1.0-1.5 mV from top of R
wave to bottom of S
wave
Masked atrial
T wave
Atrial repolarization Masked by QRS complex
Occurs 0.15-0.20 sec after
termination of P wave
QT interval (0.26-0.45)*
- beginning of Q wave to end of
T wave
J point – beginning of ST
segment
ST interval – end of QRS, start
of T
T wave
(ventricular T
wave)
Ventricular
repolarization
Occurs 0.20 sec after the
beginning of ventricular
depolarization; may take as
long as 0.35 sec
0.2 – 0.3 mV
Heart Rate – reciprocal of the time between two successive heartbeats; =1500/#lines from 0 to R
10
CHAPTER 12
ELECTROCARDIOGRAPHIC INTERPRETATION OF CARDIAC MUSCLE AND CORONARY BLOOD FLOW ABNORMALITIES: VECTORAL
ABNORMALITIES
PRECORDIAL CHEST LEADS ATTACHMENT
V1 4
th
ICS right; parasternal border
V2 4
th
ICS right; parasternal border
V3 Between V2 and V
V4 5
th
ICS; midclavicular line
V5 5
th
ICS; anterior axillary line
V6 5
th
ICS; left mid-axillary line
Lateral leads – aVL, V 5
, V
6
, I
Inferior leads – aVF, II, III
Anterior leads – V 1
, V
2
Septal leads – V 3
, V
4
Factors that shift the mean electrical axis of the ventricles to the left:
Changes in the position of the heart (ie expiration, recumbent position)
Accumulation of abdominal fat – presses upward on the heart
Left BBB – impulse spreads to right ventricle 2-3x as fast as in the left ventricle
Hypertrophy of the left ventricle – caused by hypertension, aortic valve stenosis, aortic valvular regurgitation
Factors that shift the MEA of the ventricles to the right:
Inspiration
Standing up
Lack of abdominal fat – heart rotates CW
Right BBB
Right ventricular hypertrophy